Patella Luxation
Medial Patella Luxation
The canine stifle (knee) is a complex joint with the femur rotating over the tibial plateaux. The patella (knee cap) runs in a groove over the top of the femur and acts as a pulley attached to the quadriceps muscles forming the quadriceps mechanism which is responsible for weight bearing in the hindlimb.
What is medial patella luxation?
In a number of breeds of dog (both large and small) the patella slips medially (the inside) as the stifle is flexed and extended which causes both pain and discomfort and leads to Osteoarthritis. It is caused by abnormal forces exerted through the quadriceps mechanism which pull the patella off the side rather than just back and forth.
The reason for MPL is usually because of a number of deformities that occur as the leg develops, these may include bowing and twisting of the femur and tibia and twisting and rotation of the insertion of the patella ligament onto the tibia. There may be other abnormalities as well such as twisting of the tibial shaft and an abnormal patella position within the groove (patella alta). Because the patella does not stay in position the groove does not develop properly and may be shallow. AS the patella slips back and forth the cartilage on the ridge of the trochlear grove and the underside of the patella start to wear out and this may also have a significant impact on the cause of pain, once cartilage is lost it cannot return as normal hyaline cartilage.
The degree of MPL is judged on a scale (1 to 4). Severe cases where the patella is always luxated and cannot be easily repositioned are graded 4, cases where the patella only occasionally comes out but spontaneously returns are graded 1. The grade of luxation is important as it has a direct influence on prognosis with surgery.
Clinically the signs you see depend on the grade of MPL and whether there are significant other problems such as Osteoarthritis (OA) and cruciate injury. The lameness caused by patella luxation can be caused by the physical luxation and change of normal mechanics of the knee joints and or can be caused by the secondary OA, determining the extent of the patellofemoral joint OA is therefore important as in some cases this may be such that it causes more pain than the luxation itself.
Grade ¼ cases will only occasionally skip along on three legs, grade 2/4 cases will spend more time lame and may show signs of arthritis (pain and stiffness especially after rest). Grade 4/4 cases are usually very severely debilitated because the secondary changes present will prevent the patella from returning to the groove it should run in, in these cases there may be very severe OA present. In a small number of dogs the patella may not be luxating (because they have had previous surgery to correct this) but the joint may have become severely arthritic with little cartilage left in the patellofemoral joint.
On the whole MPL is progressive, that is to say cases that have grade 1 as young dogs will go on to develop a worsening grade as they get older and because of the intermittent luxation damage will occur to the underside of the patella and arthritis will develop. Treating patella luxation early will hopefully prevent or slow down some of the other secondary problems and will prevent the grade of luxation from getting worse, for this reason we advocate early surgical intervention and we also believe that dogs that show very early signs in the other leg should be carefully considered for prophylactic surgery (treatment to prevent a problem developing in the future rather than treatment for a current problem).
Investigations
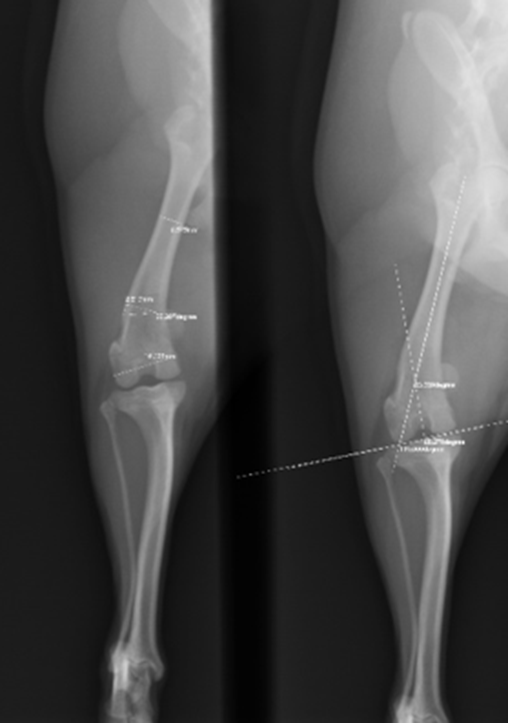
Careful clinical examination will help to determine the grade of luxation and we will normally arrange to take X rays of your dog’s legs before performing surgery. This allows us to make a full assessment of the problem and so determine the best course of treatment, in some circumstances we may arrange for a CT scan to be performed in order to determine more accurately where the bends and twists are and how sever they are in order to address these directly.
Because the extent of cartilage damage can be directly related to the long term prognosis an arthroscopic (keyhole) examination of the femoropatella joint is often worthwhile. This also allows us to assess the depth of the trochlear groove, this can be done at the same time as elective surgery described below, however if extensive OA is found we may need to consider more extensive surgery such as patella groove replacement (PGR).
Treatment
Elective treatment for most cases is aimed at re- aligning the quadriceps mechanism to reverse the pull on the patella causing the luxation and deepening the groove that the patella runs in if required. These procedures may include:
- Tibial tubercle transposition. This is a simple procedure that involves moving the insertion point of the patella ligament to simply realign the quadriceps. It is often all that is required in many grade 1 and 2 cases.
- Tibial osteotomy to correct patella alta. This is a far more invasive surgery as it involves cutting the weight bearing axis of the tibia.
- For dogs that have a significantly shallow groove this should be addressed at the same time by trochlearplasty.
Advanced Surgery
More advanced surgery may be necessary if there is significant bending and twisting of the femur or if the grade of luxation is high (grade 3 and 4) or if significant OA is seen.
Femoral Osteotomy
This is a procedure in which a wedge of bone is cut out of the end of the femur in order to correct the amount of bowing which is contributing to the luxation. The controlled femoral fracture is then plated to stabilise and heal which takes 8 to 12 weeks. This is a significantly more invasive surgery than tibial crest transposition but provides a more reliable correction in higher grade luxations and in dogs with significant femoral varus (bowing).
Patella groove Replacement (PGR)
PGR is a new technique that we believe holds significant promise for treatment of dogs that have severe patellofemoral OA. It involves replacing the trochlear groove with an entirely synthetic wear surface which removes the source of OA pain and helps control the luxation.
Cases that have PGR require very careful post operative control, the surgery is a major open procedure and as it is a partial joint replacement procedure critical care must be taken to minimise possible problems (once the part has been replaced it cannot be put back).
In all cases careful control after surgery by caged confinement is important to minimise the risk of implant failure and fracture until the bone has healed (typically 4 to 8 weeks). Careful physiotherapy plays an important role during this time and after and a full return to function should not be expected for 12 to 16 weeks.