Cranial Cruciate Disease
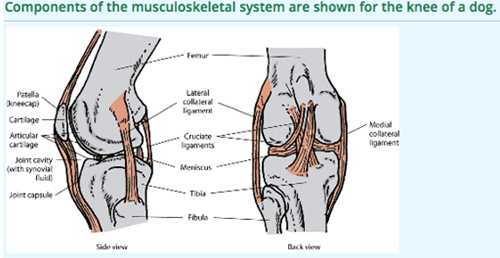
A dog’s knee joint is not unlike our knee joint but is called the stifle. The stifle joint is made up of the femur, the tibia and patella, with ligaments and structures holding it together and muscles acting on it by tendons. Although we do sometimes see fractures of the bones the majority of problems in dog knees are to do with the cruciate ligament and on occasion the collateral ligaments and menisci.
- The collateral ligaments. These are two ligaments either side of the stifle and prevent the joint unhinging either side.
- The cruciate ligaments. These are two ligaments that run through the joint, crossing over in the middle. These prevent the joint rocking backwards and forwards.
- The menisci. These are two cartilages within the joint that act as buffers between the femur and tibia.
- The joint capsule and muscles around the joint.
The single most common cause of hindlimb lameness in the dog is caused by degeneration to the Cranial Cruciate Ligament (CCL).
The condition has a variable presentation, most dogs are usually intermittently lame or stiff for some time before and then suddenly become very lame for no apparent reason (turning around in the garden) when they rupture the ligament. Some dogs present with a very gradual worsening of lameness and some dogs present early on in the condition. Any breed of dog can develop this condition usually in middle age but some breeds of dog have become associated with the condition developing early in life (Rottweiler, Labrador, Newfoundland). In a very small number of cases the cruciate ligament may become ruptured through a traumatic incident and there are often other injuries at the same time such as damage to the collaterals and or the caudal cruciate ligament, in these cases the management will involve surgery to stabilise the joint but the prognosis is often very different.
When the cruciate ligament starts to fail or suddenly fails the cause of pain will be different in different dogs but the cause of pain may include:
Instability
Because the cruciate ligament gives the stifle joint a great deal of stability, if it tears or ruptures then the joint becomes unstable, however the degree of instability will be affected by how slowly the cruciate ruptures and how the body has been able to adapt and also by how much the cruciate ruptures.
Osteo Arthritis
Because the cruciate ligament will have been failing there will already be some degree of OA present. The extent of OA and to what extent it will cause problems will be determined by X rays and also examining the joint but the vast majority of dogs will be able to manage their OA long term.
Other injuries, the meniscus and joint cartilage
The two C shaped “cartilages” within the stifle are important buffers between the rounded femur and relatively flat tibia, when the stifle is unstable to any degree the medial (inside) meniscus is at particular risk of becoming torn. These tears can be a source of considerable pain as the free torn portion will become trapped between the femur and tibia during normal movement. This torn part can also result in further damage to the articular cartilage, it is vital that the meniscal cartilages are examined and any torn part removed, in some cases we may elect to “release” the meniscus so that it cannot become damaged in the future and in a very small number of cases the meniscus may be repaired.
Determining the cause of the lameness is very important as it will help direct us to how best to treat your dog. For the vast majority of dogs, surgery will provide the best option to get back to as near normal as possible.
Investigations
The starting point for all cases is a detailed clinical examination and discussion of your dog’s history. This allows us to rule out other causes of lameness and decide, as a team, how best to proceed forward for your pet as an individual. What is right for one dog may be different for another.
Once we have determined that the stifle is the source of pain and we have carefully ascertained how unstable the joint is we will then always take X rays. Your vet may well have taken some X rays already but it is very important that we take the specialist views we need to make measurements and at the same time we determine how unstable the joint is whilst deeply sedated. Occasionally we may also arrange a CT scan which allows us to make a better 3D assessment of the bones.

Once X rays have been taken and angles and measurements made, we will discuss the best options available to treat your dog. Surgery is aimed to address as many aspects of the cause of lameness (instability, OA, other joint injury and meniscal tears) as possible in order to get the best outcome for your dog. Every surgical case will therefore need the joint to be examined in detail and arthroscopy is without doubt the best way to achieve this. At Ridge Referrals we routinely perform arthroscopy on dogs as large as 100kg and as small as 3kg, not only do we have the equipment to do this but also the expertise to do so. This is something that very few referral practices in the UK can offer. What we don’t do is apply just one treatment to every case that comes through the door.
Arthroscopy of the Stifle
This is a surgical procedure and we will typically perform the arthroscopy first and then proceed straight away with any other surgery. The arthroscopy is aimed at examining the entire joint (not something that can be done via a standard open arthrotomy) so that any damage to the meniscus can be addressed, the extent of cruciate injury confirmed and also document the extent of other injuries to the joint, especially if there is significant cartilage injury. In cases where we suspect that the cruciate has early tearing we need to confirm this unequivocally before embarking on further surgery and in a very small number of cases the extent of cartilage injury is such that we believe further surgery may not have much benefit. There is a small subset of dogs that have extensive OA affecting the knee because the cruciate ligament has failed over a prolonged period of time, if this is the case and there is a significant meniscal injury then arthroscopic surgery to trim the meniscus may be all that is needed.
|
Joint stabilisation
- Dogs that have unstable knees, in other words the cruciate ligament has completely failed, we must restore more normal stability to the joint. This can be achieved by either placing strong suture materials outside the knee joint to mimic the function of the cruciate ligament (isometric suture stabilisation) or change the mechanics of the joint so that the knee is stable when the dog places weight through its leg. (tibial plateaux levelling osteotomy or TPLO).
- The isometric suture technique is called a Tightrope. It is generally more successful in smaller patients but cannot be used if the tibial plateaux angle is higher than 28 degrees.
- The TPLO procedure involves cutting the tibia and changing the mechanics of the stifle joint.

- Just which case is better suited to the TPLO or the suture technique depends on a great deal of factors including age, activity levels, size, joint mechanics and individual owner factors. We have extensive experience in both techniques and both techniques have their pros and cons, as a general guide we feel that medium and larger breed dogs with previous high activity levels will do better with TPLO.
- Many years ago attempts to reconstruct the cruciate ligament in dogs that had completely ruptured, as is done for people were shown to be unsuccessful, more recent attempts with better materials have continued to fail. However if the cruciate ligament is partially torn then we have been able to show that the functional remnants can be saved with the TPLO procedure. Arthroscopy is vital to these cases to be able to show that the cruciate ligament is just starting to fail as the clinical signs may be subtle. Early intervention in these cases is we believe fully justified as we can “save” the early partial cruciate tears.
- In some dogs the TPLO procedure combined with an isometric suture is needed, this is called the internally braced TPLO and is generally required for dogs that have had a very sudden onset of rupture and a very unstable knee joint.
- In dogs with a chronic cruciate rupture and extensive secondary stabilisation the cause of lameness is often and meniscal tear and stifle arthroscopy to confirm this and debride the tear is all that is required.
- In a small number of dogs the cruciate ligament may fail and this may worsen a pre existing patella luxation. These are complex cases but the basic principles of both addressing the cruciate rupture and the patella luxation together are used.

Physiotherapy
Properly supervised and demonstrated physiotherapy is of great benefit to your dog in the immediate post operative period. Some very simple things should be done in the first few weeks after surgery such as icing but no active physio should be started for 6 weeks, after this time an appointment with the physio here (or we can provide you with list of suitably qualified physio in your area) has a number of benefits:
- Because we cannot ask your dog to walk in a controlled way (such as with crutches as we would be), we have to confine your dog to stop him or her doing too much. Starting some controlled static physiotherapy allows you to interact with your dog in some form of activity which is beneficial mentally to your dog.
- The static exercises are designed to maintain muscle tone and bulk, range of movement and joint function whilst your dog is recovering from surgery, preventing these from being lost means that the recovery is quicker and more effective.
- Because we are all different, we all have different requirements and so regular reassessment with the physio means that the rehab protocol can be tailored to your dog’s personal requirements.
- For high performance dogs we can consider earlier start to active physio
It is vital that physiotherapy is performed by a suitably qualified person, in appropriate physio is dangerous. The only qualification we recognise is that of a veterinary surgeon or an ACPAT Cat A physiotherapist.
POST SURGICAL CARE FOR TIGHTROPE PATIENTS
We want your dog to have the best possible outcome after his/her TightRope surgery and your role in the postoperative care is CRITICAL to success! Please follow these instructions exactly and call us right away if you are having problems in doing so.
- Please do not let your dog lick or chew at his/her incision sites at all. An Elizabethan Collar MUST be worn at all times until the incisions have healed well and we are able to take the sutures out. Please check the incisions each morning and evening for any swelling or drainage.
- Your dog should be strictly confined for the first 6-8 weeks following surgery. 1) Your dog should be in a crate 24/7. 2) You may take your pet outside on a short lead for toileting (100yds) into the garden and then back in. No other activities such as running, jumping, flexi-lead activity, stairs or playing of any type are allowed. These restrictions are necessary to allow the knee to heal well and provide the long term, pain free function we are working to achieve.
- After the first initial 6-8 weeks you will have a check up appointment with Patrick Ridge, if your dog is using his/her leg well at that point the lead controlled exercise will be gradually built up over a period of another 6 to 8 weeks. Physiotherapy should be started under the direct supervision of an ACPAT physio or veterinary surgeon.
- No unrestricted/off lead or unobserved activities are allowed until at least 16 weeks post op after which time a return to normal should be slow and over another 4 weeks
- Do not expect your dog to be back to normal for at least 16 weeks
- During the 6 – 8 week confinement period, it is recommended that your dog be given a reduced portion of his/her normal food amount to prevent weight gain.
- It is very important that you complete the prescribed medication regime when you go home. The medications help with inflammation and pain relief after surgery and decrease the risk for infection. If you feel that your dog suddenly becomes painful, has an abrupt change in limb use, or is experiencing side effects from the medications, please contact us as soon as possible.
POST SURGICAL CARE FOR TPLO
We want your dog to have the best possible outcome after his/her surgery and your role in the postoperative care is CRITICAL to success! Please follow these instructions exactly and call us right away if you are having problems in doing so.
- Please do not let your dog lick or chew at his/her incision sites at all. An Elizabethan Collar MUST be worn at all times until the incisions have healed well and we are able to take the sutures out. Please check the incisions each morning and evening for any swelling or drainage.
- Your dog should be strictly confined for the first 6 to 8 weeks following surgery. 1) Your dog should be in a crate 24/7. 2) You may take your pet outside on a short lead for toileting (100yds) into the garden and then back in. No other activities such as running, jumping, flexi-lead activity, stairs or playing of any type are allowed. These restrictions are necessary to allow the knee to heal well and provide the long term, pain free function we are working to achieve.
- After the first initial 6 to 8 weeks you will have a check up appointment with Patrick Ridge and an X ray will be taken under sedation or general anaesthesia, if the X ray shows good bony healing at that point the lead controlled exercise will be gradually built up over a period of another 6 weeks. Physiotherapy should be started under direct supervision of an ACPAT physiotherapist or veterinary surgeon.
- No unrestricted/off lead or unobserved activities are allowed until at least 12 to 14 weeks post op after which time a return to normal should be slow and over another 4 weeks
- Do not expect your dog to be back to normal for at least 16 weeks
- During the 6-8 week confinement period, it is recommended that your dog be given a reduced portion of his/her normal food amount to prevent weight gain.
- It is very important that you complete the prescribed medication regime when you go home. The medications help with inflammation and pain relief after surgery and decrease the risk for infection. If you feel that your dog suddenly becomes painful, has an abrupt change in limb use, or is experiencing side effects from the medications, please contact us as soon as possible.